Journal of Pharmaceutical Research
DOI: 10.18579/jopcr/v25.i1.129
Year: 2026, Volume: 25, Issue: 1, Pages: 29-33
Original Article
Megha Naik1, Smita Anand Tiwari2*, Sangeeta Dabhade3
1Junior Resident, Department of Pharmacology, Byramjee Jeejeebhoy Government Medical College and Sassoon General Hospital, Pune, 411001, Maharashtra, India
2Associate Professor, Department of Pharmacology, Byramjee Jeejeebhoy Government Medical College and Sassoon General Hospital, Pune, 411001, Maharashtra, India
3Professor & HOD, Department of Pharmacology, Byramjee Jeejeebhoy Government Medical College and Sassoon General Hospital, Pune, 411001, Maharashtra, India
*Corresponding Author
Smita Anand Tiwari
Email: [email protected]

Polypharmacy is common among the elderly due to multiple comorbidities, increasing the risk of drug-drug interactions, toxicities, and adverse reactions. Prescription analysis is essential to ensure rational drug use and to minimize medication- related complications. This study evaluates the rationality of geriatric prescriptions and identifies issues related to excessive medication usage using Phadke’s criteria. An observational study was conducted in the inpatient department of a tertiary care hospital. A total of 144 prescriptions were analyzed using Phadke’s criteria, which assigns score up to 30 points. Prescriptions were graded as rational (25-30 points), semi-rational (15-24 points), or irrational (0-14 points) based on adherence to clinical guidelines. The study included 144 patients with mean age 71.94 ± 6.08 years; of which 24.3% were men and 75.6% were women. Among the prescriptions analysed 59.7% prescriptions were deemed to be rational, 35.4% semi-rational, and 5.5% irrational. The most frequently prescribed medications were Pantoprazole 98.6% and Ondansetron 77.7%, with Ceftriaxone 52.1% as the most common antibiotic. Excessive multivitamin usage was also noted. Most prescriptions were rational; however, the presence of semi-rational and irrational prescriptions and the excessive medication use highlight the need for regular prescription evaluation to enhance geriatric pharmacotherapy.
Keywords: Polypharmacy, Geriatric, Prescription analysis, Rational drug use, Phadke’s criteria
The number of geriatric population (> 60 years) is increasing globally at a rapid rate with India reflecting a similar demographic trend, where 10.1% of the population is currently aged over 60 years[1, 2, 3]. This shift is primarily due to the increased life expectancy resulting from advancements in healthcare systems[4]. Such an increase in geriatric lifespan is often associated with multiple lifestyle co-morbidities resulting in polypharmacy[5-7]. Such prescriptions require careful consideration of drug–drug interactions and age-related physiological changes, which thus makes selection of appropriate medication challenging[8-10]. There is often at risk of prescribing potentially inappropriate medications (PIMs) where potential risks of medications outweigh their benefits, especially when safer or equally effective alternatives are available[6, 10]. Evidence suggests that by reducing unnecessary medications one can decrease the risk of PIMs without compromising health status[8]. Additionally factors such as self-medication, inadequate communication between prescribers and patients further exacerbates irrational prescribing, morbidity and mortality rates and also raises up the treatment costs and affects the quality of life[11, 12]. This highlights the urgent need for having a standardized criteria to that assesses the prescription rationality in geriatric patients taking into account the risk-to-benefit ratio of each prescribed medication to optimize patient care. The American Geriatrics Society (AGS) Beers Criteria are widely used to identify potentially inappropriate medications (PIMs) in older adults, while START/STOPP and Zhan’s criteria provide guidance on prescription omissions and drugs to avoid, respectively; Phadke’s criteria, on the other hand, focus on evaluating overall prescribing appropriateness[13]. Despite the availability of these criteria, challenges still persist in addressing the complex needs of elderly patients, including altered pharmacokinetics, comorbidities, and the lack of robust clinical evidence.
A prospective observational study was conducted over a period of six months by the Department of Pharmacology in collaboration with the Department of Medicine at a tertiary care hospital in the inpatient department (IPD) setup. Ethical approval was obtained from the Institutional Ethics Committee prior to the initiation of the study. Informed written consent was obtained from all participants.
A total of 144 patients aged 65 years and above were included in the study, all of whom were admitted to the inpatient department of the Department of Medicine and prescribed more than one daily medication.
The study included indoor patients aged 65 years and above, irrespective of gender, who were admitted to the Department of Medicine and who were prescribed more than one daily medication.
Patients were excluded if they were below 65 years of age, critically ill and unable to provide informed consent, had incomplete medical records, were visiting the outpatient department (OPD), or were admitted to departments other than medicine, such as surgery, ENT, or ophthalmology.
Data collection involved accessing the indoor case papers and prescriptions of eligible patients during their stay in the inpatient department. Information regarding demographic profiles, prescribed medications, comorbidities, allergies, and contraindications was recorded in a structured data collection form.
Prescription adherence was evaluated using Phadke's criteria, which is a comprehensive method for assessing prescription rationality. The criteria utilize a 30-point scale, divided as follows:
1. Correctness of Main Drug (10 points)
First choice drug used: 100% points
Second choice drug used: 60% points
Third choice drug used: 30% points
Wrong drug used: 0% points
2. Dose, Duration, Frequency of Administration of Main Drug (10 points)
Correct formulation, strength, dose, and duration: 100% points
Inadequate dose/excess dose: 50% points
Wrong formulation: 50% points
Totally wrong dose: 0% points
3. Correctness of Complementary Drug (5 points)
First choice drug used: 100% points
Second choice drug used: 60% points
Third choice drug used: 30% points
Wrong drug used instead of proper drug: 0% points
4. Dose, Duration, Frequency of Administration of Complementary Drug (5 points)
Correct formulation, strength, dose, and duration: 100% points
Inadequate dose/excess dose: 50% points
Wrong formulation: 50% points
Totally wrong dose: 0% points
Irrational drug or drug combination: 5 points each.
Unnecessary drug or injection: 5 points each.
Hazardous drugs: 10 points each.
Unnecessary injection: 5 points each.
An irrational drug or combination is defined as one not recommended in standard pharmacology textbooks or other evidence-based sources. An unnecessary drug or injection refers to a medication that is not recommended for the specific condition, excluding rational alternatives. Hazardous or banned drugs are those listed under the "Banned and bannable drugs" section of the Voluntary Health Association of India, 2003.
Each prescription was scored based on the above criteria and categorized as follows:
Rational: 25–30 points
Semi-rational: 15–24 points
Irrational: 0–14 points
The data was entered into a Microsoft® Excel® 2021 MSO (Version 2501 Build 16.0.18429.20132). Descriptive statistical analysis was done using online Sociostats software (https://www.socscistatistics.com). Data was expressed as percentages.
Out of the 144 patients enrolled in the study, 99 patients (68.8%) belonged to 65–74 years age group, whereas 38 patients (26.4%) were between the ages 75–84 years. A smaller section comprised of 7 patients (4.8%) aged 85 years and above. The mean age of the study population was 71.94 ± 6.08 years. In terms of gender distribution109 women (75.6%) and 35 men (24.3%) were present ([Table. 1]). The comorbidity assessment showed that 68 patients (47.2%) had two or more comorbid conditions. Another 46 patients (31.9%) had a single comorbidity, while 30 patients (20.8%) had no comorbidities ([Table. 2]).
|
Variables |
|
Frequency |
Percentage (%) |
|---|---|---|---|
|
Age |
65-74 |
99 |
68.8% |
|
75-84 |
38 |
26.4% |
|
|
≥85 |
7 |
4.8% |
|
|
Gender |
Male |
35 |
24.3% |
|
Female |
109 |
75.6% |
|
Variables |
Frequency |
Percentage (%) |
|
|---|---|---|---|
| No. of comorbidities |
0 |
30 |
20.8% |
|
1 |
46 |
31.9% |
|
|
≥2 |
68 |
47.2% |
|
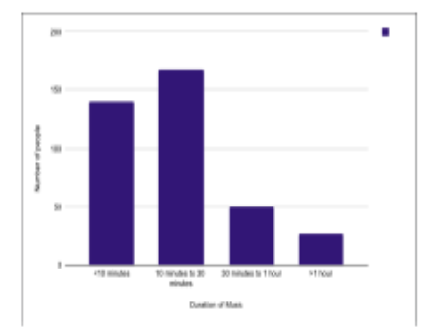
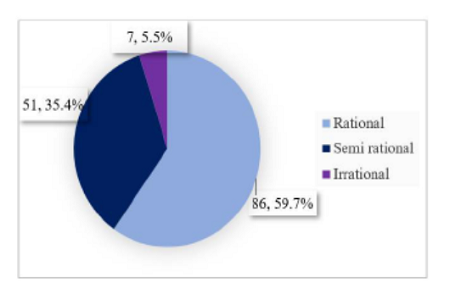
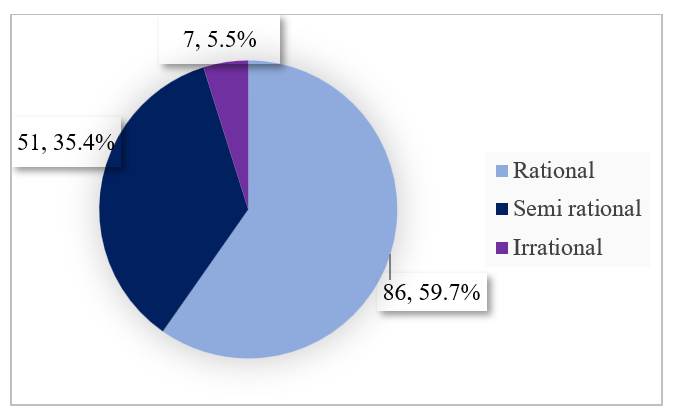
The rationality of prescriptions was assessed using Phadke’s criteria. Out of 144 prescriptions reviewed, 86 (59.7%) were classified as rational, 51 (35.4%) as semi-rational, and 7 (5.5%) as irrational ([Fig. 1]). The average rationality score across all prescriptions, regardless of their classification, was 25.38 ± 4.24.
Further analysis of the 144 prescriptions showed that 50 prescriptions (34.7%) contained a total of 59 unnecessary medications, indicating that some prescriptions included
more than one unnecessary drug. Furthermore, 23 prescriptions (15.9%) were identified to have 28 unnecessary injectable drugs, suggesting that certain prescriptions involved multiple unnecessary injectables. An irrational drug combination was also found in a single prescription (0.7%) ([Table. 3]).
|
Category |
No. of drugs |
No. of prescriptions |
|---|---|---|
|
Unnecessary drugs |
59 |
50 (34.7%) |
|
Unnecessary injectables |
28 |
23 (15.9%) |
|
Irrational drug/ combination |
1 |
1 (0.7%) |
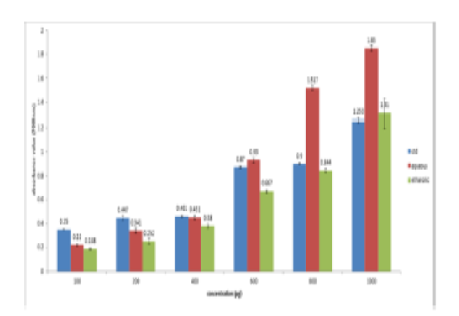
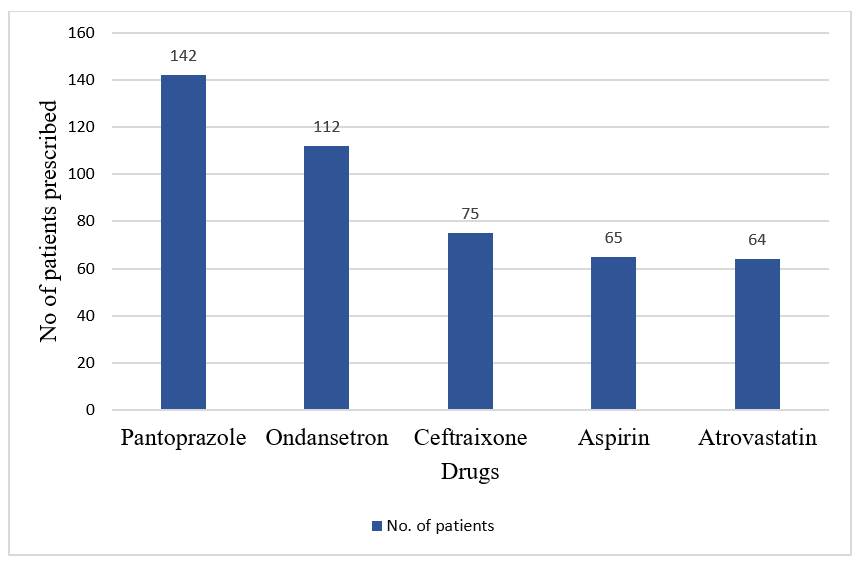
Among the most frequently prescribed medications, 142 prescriptions had Pantoprazole (98.6%), 112 included Ondansetron (77.7%), 75 had Ceftriaxone (52.0%), 68 included Aspirin (47.2%), and 64 contained Atorvastatin (44.4%) ([Fig. 2]). Ceftriaxone was the most commonly prescribed antibiotic.
The present study was conducted to evaluate the rationality of prescriptions among elderly inpatients admitted to the medicine ward of a tertiary care teaching hospital, with a focus on demographic trends, comorbidities, prescribing patterns, and adherence to standard treatment guidelines using Phadke’s criteria. In our study, the majority of patients (68.8%) were aged between 65–74 years, followed by 26.4% in the 75–84 years range, and only 4.8% aged 85 years or older. These findings are comparable to Shah et al., where 76% of patients belonged to the 65–74 age group and only 5% were above 85 years, suggesting similar age distributions across geriatric inpatient settings. Gender distribution in our study showed a female predominance (75.6%), in contrast to Shah et al., who reported a male majority (60.3%). However, Verma et al. Reported 59.9% females, supporting our observed trend.
Comorbidity assessment revealed that 47.2% of patients had two or more comorbidities, highlighting the complexity of managing elderly inpatients. This aligns with existing literature emphasizing the burden of multimorbidity in geriatric populations.
Rationality of prescriptions, assessed using Phadke’s criteria, showed that 60% were rational, 35% semi-rational, and only 5% irrational in our study. These results are more favourable compared to Shah et al., where only 39.5% prescriptions were rational and 28.3% were irrational. Patel et al. Also reported a lower proportion of rational prescriptions (16%) and a higher percentage of irrational ones (31%). The mean rationality score in our study was 25.38 ± 4.24, which was higher than Shah et al.’s 18.47 ± 9.66 and Patel et al.’s 21.4 ± 5.2. These differences in rationality outcomes may be attributed not only to varying prescribing practices and settings, but also to differences in sample size, potentially influencing the statistical outcomes. Pantoprazole, Ondansetron, Ceftriaxone, Aspirin, and Atorvastatin were the most prescribed drugs. This is consistent with Verma et al., who reported frequent use of antacids and ulcer-protective agents. Verma et al.'s findings on the frequent use of vitamins and health tonics, our study also noted an overuse of such supplements, suggesting a tendency toward non-specific prophylactic prescribing in elderly patients. Overall, the findings highlight a positive trend in rational prescription practices among elderly patients, while also indicating areas for continued improvement.
As the study was done in a tertiary care teaching hospital, majority of prescriptions in this study were classified as rational, reflecting adherence to established clinical guidelines and a generally positive approach to medication management in the geriatric population. The other findings were presence of unnecessary medications that included injectable drugs and overuse of multivitamin supplements. These findings highlight critical areas where improvement is essential to optimize pharmacotherapy and reduce unnecessary healthcare costs, which contribute to the overall economic burden on elderly patients. Such studies need to be done regularly in private healthcare setups too, where professional goals defer from that in academic institutes.
These concerns in both settings can be addressed by establishing hospital-based prescribing guidelines and ensuring strict adherence, conducting periodic prescription audits and feedback to clinicians, involving clinical pharmacists in medication review providing regular continuing medical education (CMEs) to increase awareness amongst the practitioners regarding polypharmacy, its risks and strategies to minimize it. Implementing these measures will ensure more rational use of medications, prevent redundant therapies, and promote more cost-effective and evidence-based care for this vulnerable group.
Acknowledgements: The authors gratefully acknowledge the Department of Medicine for granting permission and extending their support for this study.
Ethical approval: The study was approved by the Institutional Ethics Committee (Ref.No.: BJGMC/IEC/Pharmac/ND-062434-234) dated 26/06/24.
Funding: No funding sources.
Conflict of interest: None declared.
1. Nashiya F, Aisha H, Sapalya C, Varghese M, Bhat A. Evaluation of Prescriptions among Geriatric Patients Using Beer’s Criteria in a Tertiary Care Setting. Indian Journal of Pharmaceutical Education and Research. 2024; 58 (1s). Available from: https://doi.org/10.5530/ijper.58.1s.26
2. Dagli RJ, Sharma A. Polypharmacy: a global risk factor for elderly people. <I>Journal of International Oral Health</I>. 2014 6(6):i–ii.
3. Keche Y, Gaikwad NR, Wasnik PN, Nagpure K, Siddiqui MS, Joshi A, <I>et al</I>. Analysis of Drugs Prescribed to Elderly Patients in a Tertiary Health Care Center in Raipur, Central India: An Observational Study. Cureus. 2024; 16 (1). Available from: https://doi.org/10.7759/cureus.52770
4. Díaz Planelles I, Navarro-Tapia E, García-Algar Ó, Andreu-Fernández V. Prevalence of Potentially Inappropriate Prescriptions According to the New STOPP/START Criteria in Nursing Homes: A Systematic Review. Healthcare. 2023; 11 (3). Available from: https://doi.org/10.3390/healthcare11030422
5. Prabahar K, Alhawiti MS, Yosef AM, Alqarni RS, Sayd FY, Alsharif MO, <I>et al</I>. Potentially Inappropriate Medications in Hospitalized Older Patients in Tabuk, Saudi Arabia Using 2023 Beers Criteria: A Retrospective Multi-Centric Study. Journal of Multidisciplinary Healthcare. 2024; Volume 17 Available from: https://doi.org/10.2147/jmdh.s461180
6. Sharma R, Bansal P, Garg R, Ranjan R, Kumar R, Arora M. Prevalence of potentially inappropriate medication and its correlates in elderly hospitalized patients: A cross-sectional study based on Beers criteria. Journal of Family and Community Medicine. 2020; 27 (3). Available from: https://doi.org/10.4103/jfcm.jfcm_175_20
7. Bhagavathula AS, Vidyasagar K, Chhabra M, Rashid M, Sharma R, Bandari DK, <I>et al</I>. Prevalence of Polypharmacy, Hyperpolypharmacy and Potentially Inappropriate Medication Use in Older Adults in India: A Systematic Review and Meta-Analysis. Frontiers in Pharmacology. 2021; 12 Available from: https://doi.org/10.3389/fphar.2021.685518
8. Caçador C, Teixeira-Lemos E, Oliveira J, Pinheiro J, Teixeira-Lemos L, Ramos F. The Prevalence of Polypharmacy and Potentially Inappropriate Medications and Its Relationship with Cognitive Status in Portuguese Institutionalized Older Adults: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19 (5). Available from: https://doi.org/10.3390/ijerph19052637
9. Verma RC, Singh A, Dixit RK. Pattern of drugs prescribed for elderly patients by private practitioners of modern medicine in Lucknow, the capital of Uttar Pradesh. International Journal of Pharmaceutical Sciences and Research. 909-912; 15 (3). Available from: https://doi.org/10.13040/IJPSR.0975-8232.15(3).909-12
10. Jhaveri BN, Patel TK, Barvaliya MJ, Tripathi C. Utilization of potentially inappropriate medications in elderly patients in a tertiary care teaching hospital in India. Perspectives in Clinical Research. 2014; 5 (4). Available from: https://doi.org/10.4103/2229-3485.140562
11. Patel N, Desai M, Shah S, Patel P, Gandhi A. A study of medication errors in a tertiary care hospital. Perspectives in Clinical Research. 2016; 7 (4). Available from: https://doi.org/10.4103/2229-3485.192039
12. Shah RB, Gajjar BM, Desai SV. Evaluation of the appropriateness of prescribing in geriatric patients using Beers criteria and Phadke's criteria and comparison thereof. Journal of Pharmacology and Pharmacotherapeutics. 2011; 2 (4). Available from: https://doi.org/10.4103/0976-500x.85948
13. Singaravelu SL. Prescription Analysis: Detection and Auditing in Teaching Hospitals. Annals of SBV. 2018; 7 (2). Available from: https://doi.org/10.5005/jp-journals-10085-7304
© 2026 Published by Krupanidhi College of Pharmacy. This is an open-access article under the CC BY-NC-ND license (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Subscribe now for latest articles and news.