Journal of Pharmaceutical Research
Year: 2026, Volume: 25, Issue: 2, Pages: 112-115
Original Article
Jesmi James1*, Jitha Sushama2, Dhanya Sasidharan Palappallil3
1Associate Professor, Department of Pharmacology, Mount Zion Medical College, Adoor, Pathanamthitta, Kerala, India
2Professor CAP, Department of Pharmacology, Government Medical College, Thiruvananthapuram, Kerala, India
3Professor CAP, Department of Pharmacology, Government Medical College, Kottayam, Kerala, India
*Corresponding Author
Email: [email protected]

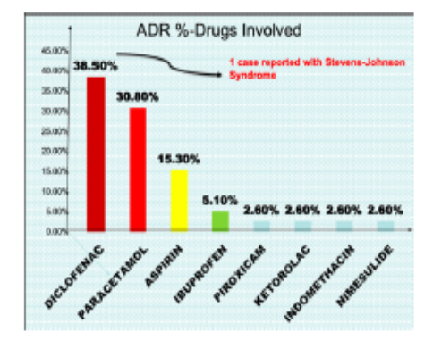
Nonsteroidal anti-inflammatory drugs (NSAIDs) are one of the most prescribed drugs in modern medicine. NSAIDs are very effective in decreasing the pain, inflammation and many patients world-wide have found relief in their use. However, they cause various side effects including cutaneous, gastrointestinal (GI) disorders (from minor dyspepsia through to major ulcers, bleeding and perforation), kidney effects and cardiovascular effects. Objective of the study is to study the pattern of Adverse Drug Reactions (ADRs) of NSAIDs in a tertiary care hospital. This was an observational study done in the Dept. of Pharmacology, Government T.D. Medical College, Alappuzha over a period of one year (July 2014- 2015). As a part of pharmacovigilance programme, all ADRs were collected in CDSCO forms and retrospective data was entered from the ADR forms. A total of 255 ADRs were identified during a one-year period, of which 39 (15.29%) cases were due to the use of NSAIDs. The age group was 31-40 years. Males were 35.9% and females were 64.1% with M:F ratio 1:1.8. The drugs involved in ADRs were Diclofenac (38.5%), Paracetamol (30.8%), Aspirin (15.3%), Ibuprofen (5.1%), Piroxicam (2.6%), Ketorolac (2.6%), Indomethacin (2.6%) and Nimesulide (2.6%). Skin was the most commonly affected organ system (71.8%), followed by GIT (15.3%), Renal (7.7%), Respiratory (7.7%) and CNS (5.1%). Causality assessment showed that 71.8% ADRs were possible and 28.2% were probable according to Naranjo’s scale. Severity assessment using the Modified Hartwig and Siegel Scale showed that 76.9% reactions were mild, 15.4% were moderate and 7.7% were severe, out of which one case was reported with Stevens-Johnson Syndrome (SJS). The causative drugs were stopped, and the patients were managed conservatively. No case fatalities were reported. Since ADRs due to NSAIDs may vary from self- limiting rash to severe life-threatening condition, the prescribing clinicians should be aware of the toxic potential of drugs and be vigilant in the spontaneous reporting the ADRs.
Keywords: Adverse Drug Reactions, Non-Steroidal Anti-inflammatory Drugs, pharmacovigilance, Naranjo’s scale, Causality assessment, Severity assessment
1. Edwards RI, Aronson JK. Adverse drug reactions: definitions, diagnosis, and management. The Lancet. 2000; 356 (9237). Available from: https://doi.org/10.1016/s0140-6736(00)02799-9
2. Reith CH. <I>Identifying predictors of adverse drug reactions and associated costs using a claims database</I>. 2002:218. [cited 14th March 2026] Available from: http//oai.dlic.mil/oai
3. Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, <I>et al</I>. A method for estimating the probability of adverse drug reactions. Clinical Pharmacology and Therapeutics. 1981; 30 (2). Available from: https://doi.org/10.1038/clpt.1981.154
4. Abdulla A, Adams N, Bone M, Elliott AM, Gaffin J, Jones D, <I>et al</I>. Guidance on the management of pain in older people. Age and Ageing. 2013; 42 (2). Available from: https://doi.org/10.1093/ageing/afs199
5. Garcia Rodriguez LA, Cattaruzzi C, Troncon MG, Agostinis L. Risk of Hospitalization for Upper Gastrointestinal Tract Bleeding Associated With Ketorolac, Other Nonsteroidal Anti-inflammatory Drugs, Calcium Antagonists, and Other Antihypertensive Drugs. Archives of Internal Medicine. 1998; 158 (1). Available from: https://doi.org/10.1001/archinte.158.1.33
6. Hernandez-Diaz S, Garcia Rodriguez A. Association Between Nonsteroidal Anti-inflammatory Drugs and Upper Gastrointestinal Tract Bleeding/Perforation. Archives of Internal Medicine. 2000; 160 (14). Available from: https://doi.org/10.1001/archinte.160.14.2093
7. Helin-Salmivaara A, Saarelainen S, Gronroos JM, Vesalainen R, Klaukka T, Huupponen R. Risk of upper gastrointestinal events with the use of various NSAIDs: A case-control study in a general population. Scandinavian Journal of Gastroenterology. 2007; 42 (8). Available from: https://doi.org/10.1080/00365520701192326
8. Mandell BF. General tolerability and use of nonsteroidal anti-inflammatory drugs. The American Journal of Medicine. 1999; 107 (6). Available from: https://doi.org/10.1016/s0002-9343(99)00370-8
9. Garcia Rodriguez LA, Williams R, Derby LE, Dean AD, Jick H. Acute Liver Injury Associated With Nonsteroidal Anti-inflammatory Drugs and the Role of Risk Factors. Archives of Internal Medicine. 1994; 154 (3). Available from: https://doi.org/10.1001/archinte.1994.00420030117012
10. Garcia Rodriguez LA, Ruigomez A, Jick H. A Review of Epidemiologic Research on Drug‐Induced Acute Liver Injury Using the General Practice Research Data Base in the United Kingdom. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy. 1997; 17 (4). Available from: https://doi.org/10.1002/j.1875-9114.1997.tb03747.x
11. Garcia Rodriguez LA, Perez Gutthann S, Walker AM, Lueck L. The role of non-steroidal anti-inflammatory drugs in acute liver injury.. BMJ. 1992; 305 (6858). Available from: https://doi.org/10.1136/bmj.305.6858.865
12. Hussaini SH, Farrington EA. Idiosyncratic drug-induced liver injury: an overview. Expert Opinion on Drug Safety. 2007; 6 (6). Available from: https://doi.org/10.1517/14740338.6.6.673
13. European Medicine Agency EMA Press Release EMEA/247323/ 2005. <I>General recommendation about NSAIDs</I>. (accessed 14 March 2026). http://www.ema.europa.eu/docs/en_GB/document_library/Press_release/2009/11/WC500014477.pdf.
14. National Institute for Clinical Excellence. <I>Guidance on the use of cyclo-oxygenase (Cox) II selective inhibitors, celecoxib, rofecoxib, meloxicam and etodolac for osteoarthritis and rheumatoid arthritis</I>. National Institute of Clinical Excellence, London, 2001; Technology Appraisal Guidance No. 27.
15. Deviere J. Do selective cyclo-oxygenase inhibitors eliminate the adverse events associated with nonsteroidal anti-inflammatory drug therapy? <I>European Journal of Gastroenterology & Hepatology</I>. (2002) 14(Suppl. 1) S29–S33.
16. Bennett A, Tavares IA. COX-2 inhibitors compared and contrasted. Expert Opinion on Pharmacotherapy. 2001; 2 (11). Available from: https://doi.org/10.1517/14656566.2.11.1859
17. Clark DWJ, Layton D, Shakir SAW. Do Some Inhibitors of COX-2 Increase the Risk of Thromboembolic Events?. Drug Safety. 2004; 27 (7). Available from: https://doi.org/10.2165/00002018-200427070-00002
18. Sommet A, Grolleau S, Bagheri H, Lapeyre-Mestre M, Montastruc JL. Was the thrombotic risk of rofecoxib predictible from the French Pharmacovigilance Database before 30 September 2004?. European Journal of Clinical Pharmacology. 2008; 64 (8). Available from: https://doi.org/10.1007/s00228-008-0497-3
19. Solomon DH, Glynn RJ, Rothman KJ, Schneeweiss S, Setoguchi S, Mogun H, <I>et al</I>. Subgroup analyses to determine cardiovascular risk associated with nonsteroidal antiinflammatory drugs and coxibs in specific patient groups. Arthritis & Rheumatology. 2008; 59 (8). Available from: https://doi.org/10.1002/art.23911
20. Zopf Y, Rabe C, Neubert A, Gassmann KG, Rascher W, Hahn EG, <I>et al</I>. Women encounter ADRs more often than do men. European Journal of Clinical Pharmacology. 2008; 64 (10). Available from: https://doi.org/10.1007/s00228-008-0494-6
21. Dhikav V, Singh S, Anand KS. Newer non-steroidal anti-inflammatory drugs: A review of their therapeutic potential and adverse drug reactions. <I>Journal, Indian Academy of Clinical Medicine</I> 2002; 3:332-8.
22. Miceli-Richard C, Le Bars M, Schmidely N, Dougados M. Paracetamol in osteoarthritis of the knee. Annals of the Rheumatic Diseases. 2004; 63 (8). Available from: https://doi.org/10.1136/ard.2003.017236
23. Palappallil DS, Ramnath SN, Gangadhar R. Adverse drug reactions: Two years' experience from a tertiary teaching hospital in Kerala. National Journal of Physiology, Pharmacy and Pharmacology. 2017; 7 (4). Available from: https://doi.org/10.5455/njppp.2017.7.1131212122016
24. Ramnath SN, Nair PV, Philip MM, Palappallil DS. Adverse drug reactions reported to an ADR monitoring center as a part of the Pharmacovigilance Programme of India: A retrospective analysis of 3-year data. National Journal of Physiology, Pharmacy and Pharmacology. 2023; 13 (9). Available from: https://doi.org/10.5455/njppp.2023.13.07344202323072023
25. Sharma S, Jayakumar D, Palappallil DS. Pharmacovigilance of cutaneous adverse drug reactions among patients attending dermatology department at a Tertiary Care Hospital. Indian Dermatology Online Journal. 2019; 10 (5). Available from: https://doi.org/10.4103/idoj.idoj_419_18
© 2026 Published by Krupanidhi College of Pharmacy. This is an open-access article under the CC BY-NC-ND license (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Subscribe now for latest articles and news.